Rosenkranz Prize Winner Leads Effort to Protect Health-Care Workers from COVID-19 in Under-Resourced Countries
Stanford postdoc Ashley Styczynski was working on newborn antimicrobial resistance in Bangladesh when the pandemic hit. The infectious disease physician realized she had to switch gears and began working with the ministry of health to prepare hospitals for the onslaught of COVID-19 patients.
“During my trainings on infection control in Bangladeshi hospitals, I learned that many health-care workers were paralyzed by the fear of not knowing how to protect themselves against COVID-19 while caring for patients, especially during shortages of PPE,” she said. “I think this has substantially contributed to the large number of health-care workers becoming infected during the pandemic. In fact, Bangladesh has the highest rate of physician mortality from COVID of any country.”
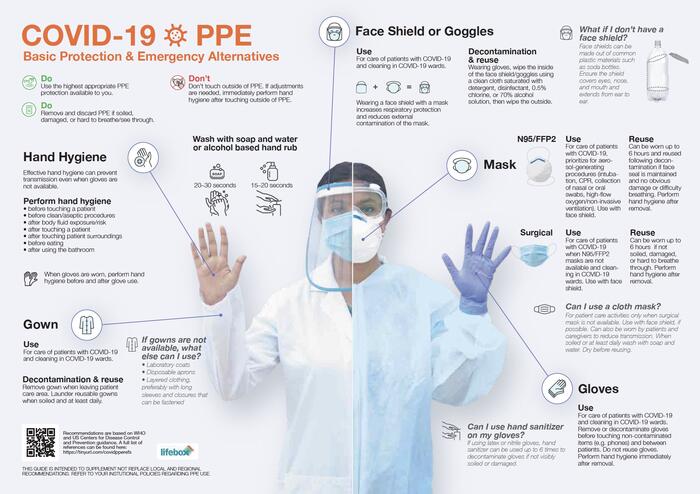
So Styczynski turned to her Stanford colleagues back home and proposed a set of infographics that could help health-care workers in Bangladesh and other under-resourced countries. Armed with a seed grant from the Stanford Center for Innovation in Global Health, they have established a website devoted to the creation and use of personal protective equipment (PPE). Bangladesh Ministry of Health has adopted their guidelines and Styczynski hopes other health ministries will do the same.
“I want them to be a tool to empower health-care workers — not just in Bangladesh but also in other low- and middle-income countries — to protect themselves with whatever resources they have access to,” Styczynski said. She said the team of collaborators from Stanford grew when researchers from other institutions heard about the research and wanted to get involved.
The website also includes a video on PPE donning-and-doffing techniques, illustrations for building ultraviolet germicidal irradiation (UVGI) cabinets to decontaminate masks, and the PPE infographics in other languages.
Stephen P. Luby, MD, a core faculty member at Stanford Health Policy and senior fellow at the Freeman Spogli Institute for International Studies and the Woods Institute for the Environment, said the project grew out of Styczynski’s background in infectious disease epidemiology and her deep engagement with collaborators in Bangladesh.
“These scientifically sound, easy-to-understand visuals provide a clear example of how deep engagement in a high-need context allows Stanford researchers to make contributions that impact lives globally,” Luby said.
Styczynski is this year’s Rosenkranz Prize winner for her ongoing research into why Bangladesh is among the top 10 countries with the highest number of stillbirths. She believes intrauterine infections may be an underrecognized factor contributing to the stillbirths and is performing metagenomic sequencing on placental tissues of stillborn babies to examine the genetic and bacterial diversity.
She recently returned to the States to marry her now-husband, Adam Gsellman, a graphic designer who did all the infographics pro bono for the project. Styczynski met him in Bangladesh, where he was working at an IT startup focused on developing travel management software.
“After having lived in Bangladesh for nearly 6 years, he is intimately connected to the country and cares deeply about the people there as well,” she said.
Other Stanford faculty involved in the project include bioengineer Manu Prakash, one of the inventors of the cheap paper microscope, the Foldscope, now used around the world, and Thomas Baer, director of the Stanford Photonics Research Center.
During the initial planning stages, Styczynski connected with Thomas Weiser, MD, MPH, a general and trauma surgeon at Stanford Medicine and the consulting medical officer for Lifebox, a nonprofit working to improve surgical safety in resource-limited settings.
"Lifebox's work is focused on infection prevention in surgery, including decontamination of surgical instruments and appropriate PPE use for surgery,” Weiser said. "We had experience doing this in the operating room, so with Ashley's help we expanded the work to include other health-care workers at risk of infection."
He added that COVID-19 presented them with additional challenges.
"But we felt it was important to prepare the surgical ecosystem to help respond to the new demands for PPE and decontamination processes that would need to be put in place," he said.

Ashley Styczynski
Read More




Stanford postdoc Ashley Styczynski and collaborators build a website devoted to protecting health-care workers in under-resourced countries, using infographics and videos to show them how to create, wear and preserve personal protective equipment.
 Rosenkranz Prize Winner Ashley Styczynski takes specimen samples with women in Dhaka, Bangladesh, for her research on antimicrobial resistance in newborns. This research led to her prize-winning proposal to investigate the alarmingly high rate of stillbirths in the South Asian nation.
Rosenkranz Prize Winner Ashley Styczynski takes specimen samples with women in Dhaka, Bangladesh, for her research on antimicrobial resistance in newborns. This research led to her prize-winning proposal to investigate the alarmingly high rate of stillbirths in the South Asian nation.
 Ashley Styczynski goes through a thermoscanner was when I was testing out the triage system at an upazila health complex.
Ashley Styczynski goes through a thermoscanner was when I was testing out the triage system at an upazila health complex.


 is the 2018 winner of the Rosenkranz Prize, which will allow him to work on developing a malaria vaccine for pregnant women. He is with Ricardo T. Rosekranz, son of Dr. George Rosenkranz, whose family endowed the prize in 2009.")
